
The Athlete
Drug Abuse
Alcohol Addiction
For about 10% to 12% of the 140 million adults in the United States who drink, the use of alcohol has developed into addiction. The incidence of alcoholism in men is approximately two to three times greater than in women (14% of male drinkers vs. 6% of female drinkers). In addition onset of alcoholism usually occurs at a younger age in men than in women (SAMHSA, 1998). In terms of consumption 20% of drinkers consume 80% of all alcohol (Greenfield & Rogers, 1999).
CLASSIFICATION
Early Classifications
Over the years there have been many attempts to classify different types of alcoholism. The purpose of classification is to develop a framework by which an illness or condition can be studied systematically rather than relying strictly on experience. According to scientific literature from the nineteenth and early twentieth centuries, researchers developed 39 classifications of alcoholics, e. g., acute, periodic, and chronic oenomania; habitual inebriety; continuous and explosive inebriate; and dipsomaniac among others.
E. M. Jellinek
In 1941 psychiatrist Karl Bowman and biometrist E. M. Jellinek presented an integration of 24 classifications of alcoholism that had appeared over the years in scientific literature. They integrated the 24 classifications into four types:
1. Primary or true alcoholics; immediate liking for alcohol and rapid development of an uncontrollable need
2. Steady endogenous symptomatic drinkers; alcoholism is secondary to a major psychiatric disorder
3. Intermittent endogenous symptomatic drinkers; periodic binge drinking, again often with a psychiatric disorder
4. Stammtisch drinkers; drinkers in whom alcoholism is precipitated by outside causes, often start as social drinkers.
Twenty years later in 1960, Jellinek in his landmark book The Disease Concept of Alcoholism proposed five types of alcoholism: alpha, beta, gamma, delta, and epsilon. Gamma and delta alcoholics were considered true alcoholics (Jellinek, 1961).
- Gamma alcoholics: mainly they have a high psychological vulnerability but also a high physiological vulnerability; they develop tissue tolerance quickly; they lose control quickly; and their progression to uncontrolled use is marked.
- Delta alcoholics: mainly they have strong sociocultural and economic influences, along with a high physiological vulnerability; they also acquire tissue dependence rapidly and it's hard for them to abstain; their progression to alcoholism is much slower than gamma alcoholism. (Babor, 1995; Jellinek, 1961)
Modern Classifications
As valuable as Jellinek's classification was, the scientific basis for alcoholism wasn't as clear cut as with other illnesses and conditions. Four developments starting in the 1950s led to a deeper understanding of alcoholism.
- First was the discovery of the nucleus accumbens, an area of the brain that gives a surge of pleasure and a desire to repeat the action when stimulated by electricity or by psychoactive drugs (Olds & Milner, 1954; Olds, 1956).
- Next was the discovery of endogenous neurotransmitters, starting in the '70s, which showed that drugs worked by influencing existing neurological pathways and receptor sites in the central nervous system including the reward pathway that researcher James Olds and others had hinted at in the '50s and '60s (Goldstein, 1994).
- In the 1980s and '90s, genetic research tools developed insights into genetic influences on addiction; in 1990 the first gene that seemed to have an influence on vulnerability to alcoholism was discovered (Noble, Blum, Montgomery, & Sheridan, 1991; Blum, Braverman, Cull, et al., 2000).
- In the '90s, imaging techniques visualized the actual reaction of the brain to drugs.
These developments took classification of alcoholism and addiction away from empirical classification to a more measurable and visible basis.
Type I &Type II Alcoholics. Based on an extensive study of Swedish adoptees and their biological or adoptive parents, type I alcoholism (also called "milieu-limited") is defined as a later onset syndrome that can affect both men and women. It requires the presence of a genetic and environmental predisposition; it can be moderate or severe; and takes years of drinking to trigger it (much like Jellenek's delta alcoholic). Type II alcoholism (also called "male-limited") mostly affects sons of male alcoho-lics, is moderately severe, is primar-ily genetic, and is only mildly influenced by environmental factors (Cloninger et al., 1996; Bohman, Sigvardson, & Cloniger, 1981).
Type A &Type B Alcoholics. T. F. Babor and his colleagues introduced the A/B typologies in 1992. They are similar to Cloninger's type I/II typologies. Type A, like type I, is a later onset of alcoholism, less family history of alcoholism, and less severe dependence. Type B, like type II, refers to a more severe alcoholism with an earlier onset, more impulsive behavior and conduct problems or disorders, more co-occurring mental disorders, and more severe dependence (Babor, Dolinsky, Meyer, et al., 1992).
The Disease Concept of Alcoholism
Much of the current research in alcohol abuse treatment is based on the disease concept. However, the idea of alcoholism as a disease goes back thousands of years but only recently has the concept become widely accepted. Both the World Health Organization and the American Medical Association view alcoholism as a specific disease entity (O'Brien, 1991). In 1992 a medical panel from the American Society of Addiction Medicine and the National Council on Alcoholism and Drug Dependence defined alcoholism as follows:
"Alcoholism is a primary chronic disease with genetic, psychosocial, and environmental factors influencing its development and manifestation. The disease is often progressive and fatal. It is characterized by impaired control over drinking, preoccupation with the drug (alcohol), use of alcohol despite adverse consequences, and distortions in thinking, most notably denial. Each of these symptoms may be continuous or periodic."
(Morse, Flavin, et al., 1992)
"I don't consider myself an alcoholic. I have five drinks a day-and that's an average. It's always three and sometimes it's a lot more but it's never interfered with my work. I haven't been to the doctor for 15 years. But since it's never interfered with my work, I see nothing wrong with sitting down and having a drink."
Avowed habitual drinker
Heredity, Environment, & Psychoactive Drugs
Instead of focusing on typologies, it is useful to look at addiction and alcoholism as a continuum of severity that depends, to varying degrees, on genetic predisposition, environmental influences due to the family, workplace, school, or community, and from the action of psychoactive drugs themselves, which can alter the body's neurochemistry and instill craving.
Family studies, twin studies, animal studies, and adoption studies are showing stronger and stronger genetic influences particularly in severe alcoholism (Nutt, 1998; Anthenelli & Schuckit, 1998; Knop, Goodwin, Teasdale, et al., 1984; Blum et al., 1996; Li, Lumeng, McBride & Chao, 1986; Goodwin, 1997). A recent twin study that assessed alcohol-related disorders among 3,516 twins in Virginia concluded that the genetic influence was 48% to 58% of the various influences, a rate much higher than postulated in the past (Prescott & Kendler, 1999). It is theorized that several genes have an influence on one's susceptibility to alcoholism and other drug addictions. A person could have one, several, or all of the genes that make a person susceptible to addiction not just a single gene such as the dopamine D2 allele receptor gene that governs the number of dopamine receptor sites in the reward pathway of the brain that signals euphoria (Blum et al., 2000). Other markers for a strong genetic influence are a tendency to have blackouts, a greater initial tolerance to alcohol, an impaired decision-making area of the brain, a major shift in personality, an impaired ability to learn from mistakes, and retrograde amnesia.
I'm an adult child of an alcoholic. I came from a long history in my family of alcoholism-my father, my mother, all of his brothers. My father died of alcoholism. So I think growing up in that environment was very depressing and so I think I was depressed for a long time and didn't know it.
43-year-old recovering alcoholic
For other people, the environmental factors are the overwhelming influences: child abuse, poverty, poor nutrition, alcohol and other drug-abusing friends and relations, and extreme stress.
"When I was younger I was always surrounded by alcohol and drugs. My mom was an alcoholic, my sister used, and so did my two stepbrothers and stepsister. My stepdad also used to grow [marijuana]. So I was kind of around it a lot. "
19 -year-old recovering alcoholic
And for some the physiological effects of alcohol and other drugs change neurochemistry and are most important.
"After a while it got to the point where I didn't care what it tasted like. You just wanted that buzz to keep going. The brain was craving alcohol. It was the hard liquor and the higher volume of alcohol involved with it, I think. To this day I still like the taste of Jack Daniels and I watch myself real close."
Recovering 32-year-old alcoholic
In the end what is important varies with the point of view of the person involved. To a researcher or scientist, classification and a systematic view of the science of alcoholism is important. To a psychiatrist, counselor, or social worker, the causes and chemistry of addiction are important because they lead to strategies to counteract craving and lack of control. To the problem drinker or alcoholic, any help, knowledge, or methods that will keep them sober and lessen the craving are important. To all involved, understanding the harm that chronic use can cause is important.
LONG-TERM EFFECTS OF ADDICTION (alcoholism)
Most psychoactive drugs affect a single type of receptor or neurotransmitter, i.e., anandamide receptor for marijuana; endorphin receptor for heroin; or norepinephrine, epinephrine, and dopamine neurotransmitters for cocaine. Alcohol on the other hand interacts with receptors, neurotransmitters, cell membranes, intracellular signaling enzymes, and even genes. Therefore the effect of long-term alcohol abuse on neurochemistry and cellular function is wide-ranging and profound (NIAAA/Congress, 1997).
Liver Disease
Since 80% of the alcohol drunk passes through the liver and must be metabolized, high-dose and chronic drinking inevitably affect this crucial organ. In the United States approximately 10% to 35% of heavy drinkers develop alcoholic hepatitis while 10% to 20% develop cirrhosis (NIAAA, 1993).
Alcoholic hepatitis causes inflammation of the liver, areas of fibrosis, necrosis, and damaged membranes. It can take months or years of heavy drinking to develop this condition, which is manifested by jaundice, liver enlargement, tenderness, and pain. It is a serious condition that can only be arrested by abstinence from alcohol but even then the scarring of the liver and collateral damage remains (Moddrey, 1988).
©1998 Pittsburgh Post-Gazette, Rogers. Reprinted, by permission. All rights reserved

Cirrhosis, the most advanced form of liver disease caused by drinking, is the leading cause of death among alcoholics. Approximately 10,000 to 24,000 Americans die each year from cirrhosis due to alcohol consumption (DeBakey, Stinson, Grant, & Dufour, 1996). When alcohol kills liver cells, the tissues do not regenerate, they scar. The damaging effects of alcohol occur not only because alcohol itself is toxic but because the metabolic process produces metabolites, such as free radicals and acetaldehyde, that are even more toxic than alcohol itself (Kurose, Higuchi, Kato, Miura, & Ishii, 1996). Cirrhosis, like alcoholic hepatitis, is not amenable to treatment although abstinence can often arrest the progression of the disease.

This fatty liver of a drinker is caused by accumulation of fatty acids. When drinking stops, the fat deposits usually disappear. Courtesy of Boris Ruebner, MD. Cirrhosis of the liver takes 10 or more years of steady drinking. The toxic effects of alcohol cause scar tissue to replace healthy tissue. This condition remains permanent, even when drinking stops. Courtesy of Boris Ruebner, MD.

"I would have taken better care of my body if I knew I would live this long."
Mickey Mantle
Mickey Mantle's liver failed because of heavy drinking and cancer. He had a liver transplant but the cancer had spread throughout his body. He died in 1995.
In addition accumulation of fatty acids in the liver, a condition called "fatty liver," can begin to occur after just a few days of heavy drinking. Abstention will eliminate much of the accumulated fat. When the liver becomes damaged due to cirrhosis, fatty liver, or hepatitis, its ability to metabolize alcohol decreases, thus allowing the alcohol to travel to other organs in its original toxic form. Even persistent moderate drinking can then begin to damage the liver.
Digestive System
While lower doses of alcohol can aid digestion, moderate to higher doses stimulate the production of stomach acid and delay the emptying time of the stomach. Excessive amounts can cause acid stomach, diarrhea, and peptic ulcers. Gastritis (stomach inflammation) is common among heavy drinkers as are inflammation and irritation of the esophagus, pancreas (pancreatitis), and small intestine. Serious disorders including ulcers, stomach hemorrhage, and gastrointestinal bleeding are also linked to heavy drinking (Lieber, 1998). Damage to the liver also causes problems with digestion and proper metabolism.
Alcohol contains calories (about 140 in a 12-oz. beer) but almost no vitamins, minerals, or proteins. Heavy drinkers receive energy but little nutritional value from their drinking. As a result alcoholics may suffer from primary malnutrition, including vitamin B1 deficiency leading to beriberi, heart disease, peripheral nerve degeneration, pellagra, scurvy, and anemia (caused by iron deficiency). In addition because heavy drinking irritates and inflames the stomach and intestines, alcoholics may suffer from secondary malnutrition (especially from distilled alcohol drinks) as a result of faulty digestion and absorption of nutrients, even if they eat a well-balanced diet.
Cardiovascular Disease
Though light drinking is associated with lowered risk of heart disease and stroke, chronic heavy drinking is related to a variety of heart diseases including hypertension (high blood pressure) and cardiac arrhythmias (abnormal irregular heart rhythms) (Klatsky, 1988). Heavy drinking increases the risk of hypertension by a factor of two or three. Cardiomyopathy, an enlarged, flabby, and inefficient heart, is found in heavy chronic drinkers since acetylaldehyde damages heart muscles.
One form of irregular heart rhythm is called "holiday heart syndrome" because it appears in patients from Sundays through Tuesdays or around holidays after a large amount of alcohol has been consumed. Heavy drinking increases the risk of stroke and other intracranial bleeding within 24 hours of a drinking binge (Geller, 1997). The exact mechanism for many of the cardiovascular problems is not definitely known but the connection is clear.
Nervous System
Alcohol limits the brain's ability to use glucose and oxygen, thus killing brain cells as well as inhibiting message transmission. Low to moderate use does not seem to cause permanent functional loss whereas chronic high-dose use causes direct damage to nerve cells. Malnutrition can also injure brain cells and disrupt brain chemistry.
Both physical brain damage and impaired mental abilities have been linked to advanced alcoholism. Brain atrophy (loss of brain tissue) has been documented in 50% to 100% of alcoholics (Parsons, 1977). Breathing and heart-rate irregularities caused by damage to the brain's autonomic nervous system have also been traced to brain atrophy. Dementia (deterioration of intellectual ability, faulty memory, disorientation, and diminished problem-solving ability) is a further consequence of prolonged heavy drinking.
One of the more serious diseases due to brain damage caused by chronic alcoholism and thiamine (vitamin B1) deficiency is Wernicke's encephalopathy whose symptoms include delirium, visual problems, imbalance, and muscle tremors. The other serious condition that involves thiamine deficiency is Korsakoff's syndrome; its symptoms include disorientation, memory failure, and repetition of false memories (Goodwin, 1997).
Hippocrates wrote about the association between alcohol and seizures/epilepsy more than 2,000 years ago. The prevalence of epilepsy is up to 10 times greater in those with alcoholism (Devantag, Mandich, Zaiotti, & Toffolo, 1983). While the seizures could be caused by head trauma due to drunkenness or other causes, the direct damage to neurological systems as well as the neurological storm caused by withdrawal are strongly implicated.
Reproductive System
Female. While light drinking lowers inhibitions, prolonged use decreases desire and the intensity of orgasm. In one study of chronic female alcoholics, 36% said they had orgasms less than 5% of the time. Chronic alcohol abuse can inhibit ovulation, decrease the gonadal mass, delay menstruation, and cause sexual dysfunction (Blume, 1997). Heavy drinking also raises the chances of infertility and spontaneous abortion.
Male. Again, low to moderate levels of alcohol can lower inhibitions and enhance the psychological aspects of sexual activity but the depressant effects soon take over. Chronic use causes effects beyond a temporary inability to perform. Long-term alcohol abuse impairs gonadal functions and causes a decrease in testosterone (male hormone) levels. Decreased testosterone causes an increase in estrogen (a female hormone) that can lead to male breast enlargement, testicular atrophy, low sperm count, loss of body hair, and loss of sexual desire. About 8% of alcoholics are impotent and only half can recover sexual function during sobriety. When returning to sexual activity, a recovering alcoholic may experience excessive anxiety; dysfunction can be intensified by one or two bad performances. Also alcohol may lead to increased risk-taking behavior, especially unprotected sex that leads to an increased potential for HIV and other sexually transmitted diseases.
Cancer
Breast Cancer. Although the association between drinking and breast cancer is clear, there is contradictory evidence concerning the association between drinking small amounts of alcohol and the incidence of breast cancer (see discussion earlier in this chapter under low- to moderate-dose episodes). A study of 1,200 women with breast cancer showed an association between moderate alcohol use and breast cancer-even amounts as low as one drink a day increased the risk by 50%. In fact 25% of all breast cancer is associated with even brief use of alcohol (Bowlin, 1997). However, another study said that moderate to heavy drinking was more likely to cause breast cancer (Ellison, 1999).
Other Cancers. The risk of mouth, throat, and esophageal cancer are 6 times greater for heavy alcohol users, 7 times greater for smokers, and an astonishing 38 times greater for those who smoke and drink alcohol (Blot, 1992).
Other Systemic Problems
Musculoskeletal System. Alcohol leeches minerals from the body causing a 5- to 10-fold greater risk of a fracture of the femur, the wrist, vertebrae, and the ribs. The unbalancing of electrolytes by chronic or acute use, along with direct toxic effects, can cause myopathy (painful swollen muscles).
Dermatologic Complications. The reddish complexion of chronic alcoholics is caused by rosacea, psoriasis, eczema, and facial edema, all of which are potentiated by the toxic effects of alcohol. Skin problems also arise from nutritional deficiencies.
Immune System. Excessive drinking has been linked to infectious diseases such as respiratory infections, tuberculosis, pneumonia, and cancer. Heavy drinking may disrupt white blood cells and in other ways weaken the immune system, resulting in greater susceptibility to infections.
Other Susceptibilities. Alcohol can cause a host of other problems.
- Alcohol may be a contributing cause for diabetes.
- Chronic drinking can cause atrophied muscle fibers, resulting in flabby muscles.
- It can also cause weight loss, more so for alcoholic women than alcoholic men, due to damage to the digestive system.
POLYDRUG ABUSE
Most illicit drug users drink alcohol. The reasons vary.
- Stacking: Alcohol taken before using cocaine will prolong and intensify the "coke's" effects by creating the metabolite cocaethylene, which also seems to trigger greater violence.
- Morphing: Drinking alcohol to come down off a three-day speed run.
- Multiple drug use: Taking speed to wake up, drinking at noon to relax, smoking a joint in the afternoon, and then taking alcohol to get to sleep.
- Replacement: Drinking alcohol to get loaded if the desired shot of heroin or sedative-hypnotic capsule is unavailable.
- Mixing: Drinking alcohol and shooting cocaine to get a "speedball" effect.
- Sequentialing: Switching from alcohol to another addiction when the effects of the alcohol have become too damaging; most addicts have sequenced through several addictions.
- Cycling: Binge drink for a week, and then only smoke marijuana for a week, and then back to the alcohol.
"I used downers just to come down off the alcohol because I was so shaky. And then I would try using amphetamines just to lift me up so I wouldn't drink so much. But what I would do was stay awake longer and drink more, so that didn't work."
43-year-old recovering polydrug abuser
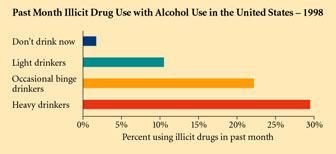
Figure 5-6. This chart shows that excessive drinking is associated witht he use of other illicit drugs, the lowering of inhibitions that makes other drug use acceptable, or the desire for stronger and stronger experiences, the association is quite clear.
Polydrug abuse has become so common that treatment centers have had to learn how to treat simultaneous addictions. Although the emotional roots of addiction are similar no matter what drug is used, the physiological and psychological changes that each drug causes, particularly during withdrawal, often have to be treated differently. For example, if a client of the Haight-Ashbury Detox Clinic has a serious alcohol and benzodiazepine problem, the Clinic has to be extremely careful detoxifying the client. That is because Librium®, a benzodiazepine sedative-hypnotic, is one of the drugs used to control the symptoms of delirium tremens caused by alcohol withdrawal.
There is a strong association between smoking and drinking. Approximately 70% of alcoholics are heavy smokers (more than one pack a day) compared to 10% of the general population. The converse is not as dramatic: smokers are only 1.3 times as likely as the general population to drink alcohol compared to nonsmokers. There is also a strong link between early use of tobacco and alcohol. Adolescents who smoke are three times more likely to begin using alcohol while smokers are 10 times more likely to become alcoholics than are nonsmokers (Shiffman & Balabanis, 1995).
Information on Drug Abuse:
Information on Alcohol:
Epidemiology of Alcohol Consumption